{kind=link}
Cluster B is one of three classifications of personality disorders defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM−5). It encompasses four distinct personality disorders that share common features related to emotional dysregulation, impulsivity, and intense interpersonal conflict.
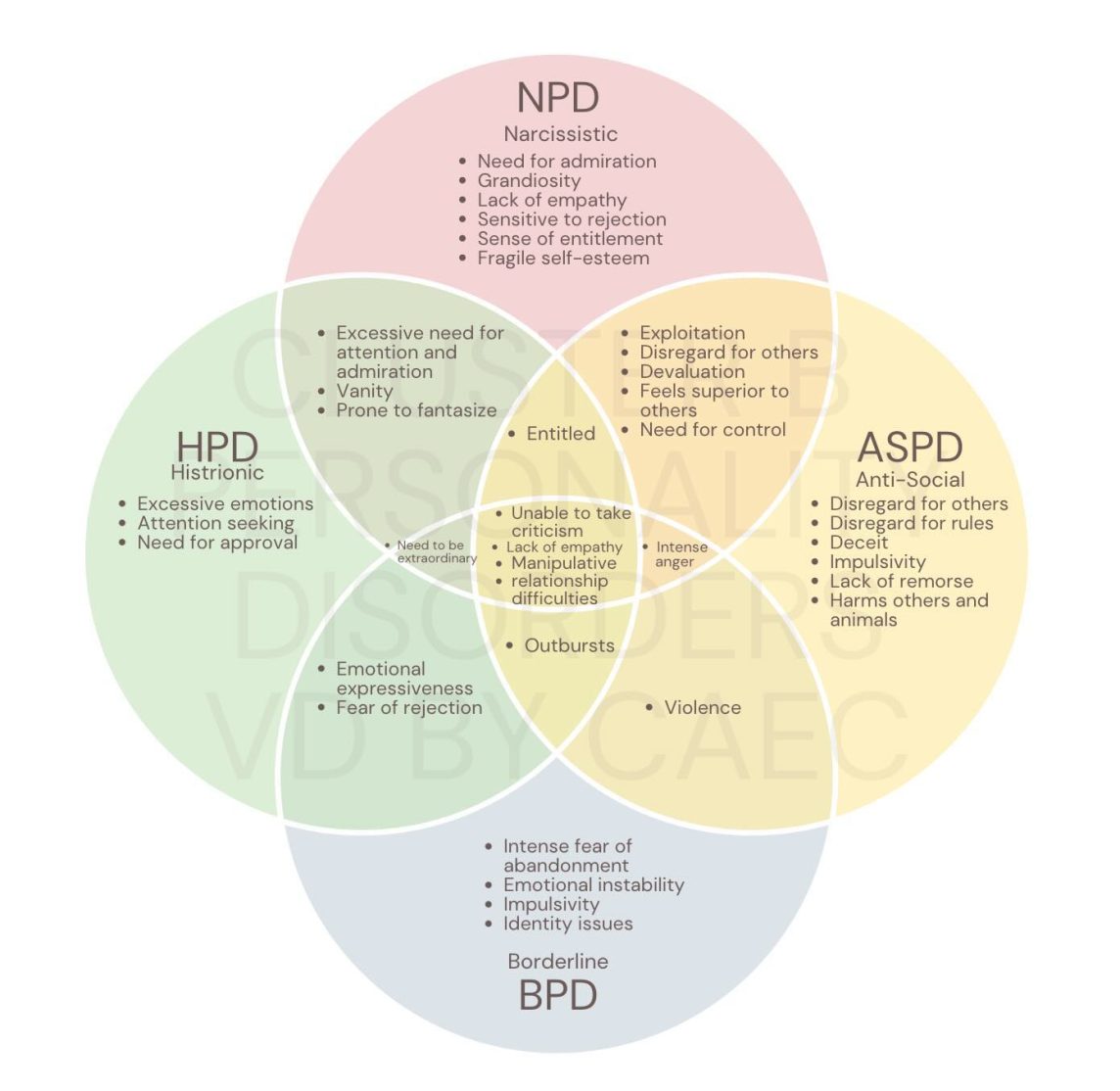
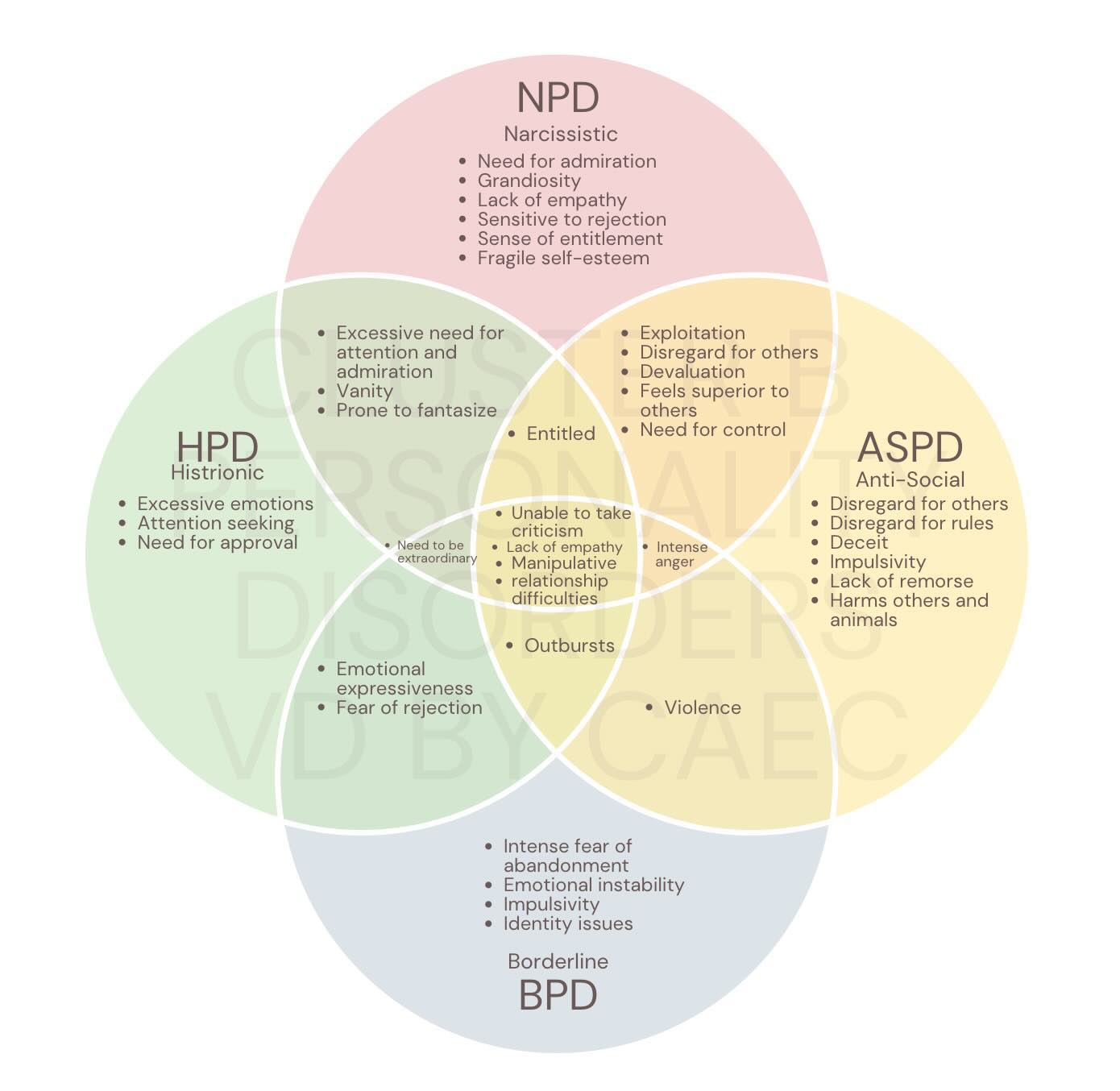
The four disorders in Cluster B are: Antisocial Personality Disorder (ASPD), Borderline Personality Disorder (BPD), Histrionic Personality Disorder (HPD), and Narcissistic Personality Disorder (NPD).
1. Signs and Behaviors by Disorder
The behaviors associated with Cluster B disorders are generally visible across four key areas of functioning: emotional responses, impulse control, interpersonal relationships, and cognition (how one perceives oneself and others).
| Disorder | Key Signs and Symptoms | Core Behaviors |
|---|---|---|
| Antisocial Personality Disorder (ASPD) | Persistent disregard for the rights of others, starting in adolescence (must be 18 years or older for diagnosis). Lack of remorse or guilt for hurting others. Deceitfulness and manipulation. | Repeatedly breaking the law or rules. Impulsive and reckless behavior, including substance abuse and dangerous driving. Lying, exploiting, and using others for personal gain without caring about the consequences. Aggressive or irritable behavior, often resulting in physical fights. |
| Borderline Personality Disorder (BPD) | Pervasive instability in moods, self-image, and relationships. Intense fear of abandonment (real or perceived). Chronic feelings of emptiness. Frequent, intense, and inappropriate anger. | Swinging views of others (often referred to as “splitting”), moving quickly between idealizing someone and intensely devaluing them. Self-harming behavior (e.g., cutting, burning) and recurrent suicidal thoughts, threats, or gestures. Impulsive actions in at least two areas (e.g., reckless spending, binge eating, unsafe sex, substance misuse). |
| Histrionic Personality Disorder (HPD) | Excessive emotionality and a pervasive pattern of attention-seeking behavior. Discomfort when not the center of attention. Shallow, rapidly shifting emotions. | Behaving dramatically or theatrically and exaggerating emotional expression. Using physical appearance or engaging in sexually provocative/seductive behavior to draw attention. Impressionistic speech that lacks detail but is highly emotional (“It was the most wonderful, amazing thing!”). Easily influenced by others or current trends. |
| Narcissistic Personality Disorder (NPD) | Pervasive pattern of grandiosity, a constant need for admiration, and a profound lack of empathy. Inflated sense of self-importance; exaggerating achievements and talents. Preoccupation with fantasies of unlimited success, power, or ideal love. | Believing they are “special” or unique and should only associate with, or be understood by, other high-status people or institutions. Sense of entitlement (expecting favorable treatment automatically). Exploiting or taking advantage of others to achieve their goals. Intense reaction (anger, shame) to perceived criticism or defeat. |
2. Common Consequences of Cluster B Behaviors
While the symptoms of each disorder are different, the shared characteristics of emotional dysregulation and impulsivity result in similar negative life consequences across the cluster.
A. Interpersonal and Relational Consequences
- Unstable Relationships: Relationships are often intense, chaotic, and short-lived, characterized by conflict, mistrust, and difficulty with intimacy.
- Social Isolation: Due to the erratic or exploitative nature of their behavior, individuals may push away family, friends, and romantic partners, leading to loneliness and isolation.
- Manipulation and Control: Behaviors are frequently geared toward controlling others, preventing abandonment, or achieving a desired outcome, leading to conflict and damaged trust.
B. Occupational and Legal Consequences
- Job Instability: Impulsivity (like quitting a job abruptly), difficulty managing conflict with authority figures, and general instability often lead to repeated job loss or difficulty advancing careers.
- Financial Distress: Reckless or impulsive behaviors (e.g., gambling, spending sprees) can result in significant debt and financial chaos.
- Legal Issues: This is particularly common in ASPD but can occur across the cluster due to impulsive behavior (e.g., reckless driving, aggression, substance misuse) leading to repeated encounters with law enforcement.
C. Physical and Mental Health Consequences
- Self-Harm and Suicidality: Especially in BPD, high rates of self-injury and suicidal behaviors require immediate clinical attention and result in frequent hospitalizations.
- High-Risk Lifestyle: Engagement in risky behaviors (e.g., substance abuse, unsafe sex, dangerous stunts) often results in accidents, injury, and negative health outcomes.
- Co-occurring Mental Health Conditions: Cluster B disorders frequently co-occur with mood disorders (like depression and bipolar disorder), anxiety disorders, eating disorders, and substance use disorders, complicating treatment and recovery.
D. Insight and Treatment Challenges
- Lack of Insight: A significant challenge is that people with personality disorders may view their own thoughts and behaviors as normal (ego-syntonic) and perceive others or outside situations as the source of the problem. This lack of insight often prevents them from seeking help or recognizing the need for change.
- Treatment Difficulty: While many Cluster B disorders are treatable with specialized psychotherapy (like Dialectical Behavior Therapy, or DBT, for BPD), engagement can be challenging due to volatile emotions, difficulty trusting the therapist, and a tendency to abandon treatment impulsively.
3. Related Concepts and Common Overlaps
Certain concepts and conditions are frequently discussed alongside Cluster B disorders due to overlapping dramatic, erratic, or deceitful behaviors.
Psychopathy (Related to ASPD)
Psychopathy is not an official DSM−5 diagnosis but is a clinical construct (often assessed using tools like the Psychopathy Checklist-Revised or PCL-R) that is highly correlated with Antisocial Personality Disorder (ASPD).
- Relationship: All individuals classified as psychopathic would likely meet the criteria for ASPD; however, not all people with ASPD are considered psychopathic.
- Distinction: Psychopathy emphasizes more interpersonal and affective traits, such as superficial charm, pathological lying, grandiose self-worth, and profound lack of empathy (callousness), in addition to the behavioral deviance central to ASPD. Psychopathy is generally considered a more severe and treatment-resistant condition.
Sociopathy (Related to ASPD)
The term “sociopathy” is not a clinical diagnosis in the DSM−5 but is often used in popular culture and sometimes by older clinicians to describe traits aligned with Antisocial Personality Disorder (ASPD).
- Usage Distinction: While often used interchangeably with ASPD, sociopathy is sometimes associated with individuals whose traits are seen as primarily the result of environmental or social factors (like childhood trauma or neglect) and may exhibit less controlled, more spontaneous antisocial behavior compared to the more calculated behavior often associated with psychopathy.
Coercive Control Abuser (Related to ASPD/NPD)
Coercive control is a pattern of behavior in domestic settings, rather than a disorder itself, but it perfectly illustrates the manipulative and dominating traits found in Narcissistic Personality Disorder (NPD) and Antisocial Personality Disorder (ASPD).
- Definition: This involves a pattern of acts (including violence, threats, intimidation, and humiliation) used to make a person dependent and subordinate. The abuser seeks to regulate and dominate nearly every aspect of the victim’s daily life.
- Cluster B Link: This behavior aligns with the lack of empathy and exploitation seen in ASPD, and the entitlement and need for absolute admiration/control seen in NPD.
Malicious Parent Syndrome (Non-Clinical Term)
This term is not recognized as a formal mental health diagnosis but is sometimes used in high-conflict legal and family court contexts.
- Definition: It describes a pattern where one parent engages in malicious and deliberate actions designed to alienate a child from the other parent, often involving false allegations or emotional manipulation of the child.
- Cluster B Link: The underlying behaviors—deceit, manipulation, lack of conscience, and using others (including a child) to achieve a personal goal (winning a custody battle or achieving revenge)—are consistent with manipulative traits found in ASPD, NPD, or high-conflict BPD presentations.
Transient Psychotic Symptoms (Related to BPD)
While true chronic psychosis (hallucinations or delusions) is characteristic of Cluster A disorders or primary psychotic disorders like Schizophrenia, individuals with Borderline Personality Disorder (BPD) can experience short-lived, stress-related episodes.
- Manifestation: These episodes typically involve transient paranoia (suspiciousness of others’ motives) or severe dissociation (feeling disconnected from oneself or reality).
- Duration: These symptoms are usually brief, lasting minutes to hours, and occur only during periods of extreme psychological distress, resolving when the stressor is removed.
Factitious Disorder Imposed on Self (Formerly Munchausen Syndrome)
Factitious Disorder is a separate DSM−5 category (a somatic symptom and related disorder), but its behaviors often align with the dramatic theme of Cluster B. The former name for the most severe form of this condition was Munchausen Syndrome.
- Definition: This disorder involves falsifying, exaggerating, or inducing physical or psychological signs or symptoms in oneself (or in another person, called Factitious Disorder Imposed on Another) to assume the sick role.
- Motivation: The primary, and often only, motivation is psychological—to gain attention, sympathy, and care from others, rather than obtaining material gain (which is characteristic of malingering). The extreme deception and dramatic presentation of illness share behavioral traits with both ASPD and HPD.